
Personal Preventive Medicine, Part 1: A Rational Guide to Lipids and Long-Term Heart Health

Motivation
My decision to take control of my own health started with this conversation I had with my doctor over two years ago:
Me: I want to start being more proactive about my health now that I’m in my thirties, and would like to do more tests than just the standard ones. For example, I’d like to do detailed hormone, lipid, and other panels.
Doctor: Not necessary, and not covered by insurance.
Me: I’m not too worried about insurance, this is important to me and I’ll pay out of pocket for whatever isn’t covered.
Doctor: Still, it's unnecessary at your age.
Me: Well I know it's not strictly necessary—but my point is I’d like to be proactive, start tracking this stuff now to develop a baseline I can monitor as I get older and hopefully get ahead of certain diseases.
Doctor: Are you getting erections in the morning?
Me: Uhmm, what? Yes, but why?
Doctor: Then your hormones are fine, you don’t need those tests at this age.
Me: The hormone panel was just one example, I also want to dig deep into more accurate lipid tests, again I’m trying to be proactive…
Doctor: I’m not going to order any of this for you. The standard tests are fine for you at this age.
Me: Okay.
That was the last time I saw that doctor. I let him run the standard tests and then found a new doctor the next year.
My next doctor was much nicer. But the philosophy was the same—if it’s not covered by insurance and there’s no immediate cause for concern, then ordering additional tests wasn't an option.
This was frustrating. Why is mainstream medicine so resistant to proactive health monitoring? Dr. Peter Attia describes this problem in his book Outlive: The Science and Art of Longevity. He calls the traditional, reactive approach "Medicine 2.0"—where doctors only treat disease after it develops. In contrast, "Medicine 3.0" is all about prevention, using data to stay ahead of health issues before they become serious (Attia, 2023).
That philosophy resonated with me. If my doctors weren’t going to support a proactive approach, I had no choice but to take matters into my own hands. I started by digging into what it really means to take a proactive approach to health—what should be measured, why it matters, and how it connects to long-term disease prevention. That research led me to order my own blood work based on the markers most supported by evidence.
This article is the first installment in a broader series on personal preventive medicine. My goal is to demystify complex medical topics and provide a logical and evidence-based framework that anyone can use to better understand their own health—starting with understanding lipids and cardiovascular risk. This isn’t a medical guide; it’s a deep-dive into the science, the metrics, and the practical steps I’ve taken to build a more proactive approach to staying healthy.
Some Background
I want to be crystal clear about what I am not: I am not a doctor, I am not a medical professional, and I am not qualified to give medical advice. But what I am qualified to do is share my own experience—what I’ve learned, what I’m tracking, and how I’m going about this process. The irony is that the very system designed to guide my health left me with no real choice but to figure it out for myself. That said, everyone’s health is different, and you should always do your own research, think critically, and rely on your doctor’s guidance. My goal with this post is to provide insight into what proactive health monitoring can look like—so you can decide for yourself how (or if) it fits into your own approach.
I am an active early 30s male with no major health concerns. In my early twenties, I was into powerlifting with some running on the side. Over time, as lifting injuries piled up, I transitioned more into bodybuilding training while increasing my emphasis on running and cardio.
Throughout my 20s, I had my blood work done about seven times. The only time my cholesterol came back high was at age 23, when I bulked up to 210 lbs on a very dirty diet (I was on a classic "see food" diet—if I saw food, I ate it—all in the pursuit of gym gains). Sure, I got strong, but my health took a hit. My cholesterol shot up, and after seeing that, I dialed things back, maintaining a weight between 180-195 lbs for the rest of my 20s. Since then, my cholesterol levels remained normal—until last year, when my total cholesterol unexpectedly hit 220 mg/dL. This scared me, but when I asked my doctor exactly what that number means and what I can do about it I got a bunch of hand-waviness and recommendations to eat a “Mediterranean diet”—whatever that means. I was already investigating proactive health, and that unexpected 220 mg/dL convinced me I had to go all-in.
Another notable experiment in my 20s was a three-year stint on a vegan diet. My blood work was mostly fine, but my B12 and D3 levels were consistently low. Supplements helped—when I actually remembered to take them.
Seeing my cholesterol spike last year (for the first time in nearly a decade) made me take a hard look at my diet and body composition. For over 10 years, I had been bulking, doing half-hearted mini-cuts, or “maingaining”—never truly prioritizing leanness or metabolic health. I had also never dropped below 15% body fat, spending most of my time in the high-teens. So, for the past six months, I made a real effort: I dropped 30 lbs (down to 155 lbs, probably slightly below 10% body fat) and started eating "healthy."
I put “healthy” in quotes because the definition of a “healthy” diet is a never-ending debate. Carnivores and vegans are both equally convinced that their way is optimal—and both have "facts" to back them up. Personally, I defined a "healthy" diet as one that is:
Mostly whole foods
Minimal processed foods
Rich in fruits and vegetables
The right total calories to maintain a healthy body weight/composition
High in protein and diverse in protein sources
My total cholesterol dropped to 180 mg/dL—which might sound like a clean bill of health. But here’s the twist: during those 90 days, I ate five eggs every single morning. That experience made me seriously question the decades-old fear around dietary cholesterol, especially from eggs. So, I dove into the research to figure out what the evidence really says. And while my total cholesterol improved, the story doesn’t end there—because total cholesterol is far from the best predictor of cardiovascular risk. In fact, some of the most important markers aren’t even included in the standard lipid panel. It’s entirely possible to have “normal” results and still be at high risk.
In this article, I’ll unpack everything I’ve learned: how to interpret lipid panels correctly, which blood markers matter the most, how lifestyle and nutrition impact cardiovascular risk, and what the science really says about eggs, saturated fat, and preventive treatment.
Understanding Cholesterol and Cardiovascular Risk
A Brief Primer
If you’ve ever looked at a cholesterol panel and felt confused, you’re not alone. Most mainstream medical conversations still rely on overly simplistic categories like “good” and “bad” cholesterol—and surprisingly, even some medical professionals still talk this way.
Despite decades of research revealing a far more nuanced picture, standard U.S. medical practices continue to focus heavily on total cholesterol and LDL-C as the core indicators of heart health. But newer evidence—and the latest guidelines from leading cardiovascular societies—tell a more complete and accurate story.
In this section, I’ll walk through that story step by step: what cholesterol actually is, which markers truly matter, and what the most up-to-date research says about assessing cardiovascular risk.
What is cholesterol?
Cholesterol is a complex carbon-based molecule. It's a type of lipid, or fat.
What does cholesterol do?
Cholesterol is absolutely vital for life and optimal health. It's a critical molecule for two very important processes:
Maintaining cell membranes. Every cell in the body relies on a healthy, functional membrane to survive and interact with its environment—and cholesterol is a key structural component of those membranes.
Synthesizing essential molecules. Cholesterol is needed for the synthesis of very important molecules including steroid hormones (like testosterone and estrogen), vitamin D, and bile acids used in digestion.
What are triglycerides?
Triglycerides are another type of lipid that is primarily used for energy storage.
What do triglycerides have to do with cholesterol?
For starters, triglycerides and cholesterol share an important chemical trait: they’re both hydrophobic, meaning they don’t mix with water. Think of sugar versus oil: you can mix sugar in water and it dissolves (it's hydrophilic), but you can’t do the same with oil (it's hydrophobic). Since blood is mostly water, both cholesterol and triglycerides need a transport vehicle in order to flow through it effectively.
What are lipoproteins?
Lipoproteins are those transport vehicles. Here’s what makes them up:
The core carries the cargo: triglycerides and cholesterol.
Phospholipids make up the shell - they have a combination of hydrophobic and hydrophilic properties which helps them hold the lipid cargo on the inside, and flow through blood easily at the same time.
Apoproteins are attached to the outside and direct the lipoprotein where to go and what to do.
Most cells in the body can synthesize their own cholesterol. Certain tissues, like the liver and intestines, synthesize a lot of cholesterol, while others, like the adrenal glands and gonads, don’t synthesize enough to meet their needs. Lipoproteins play a crucial role in shuttling cholesterol throughout the body where it is needed most. Cholesterol transport in the body is an extremely complex bi-directional traffic system, but for our purposes all that we need to know is that lipoproteins are the main vehicles ensuring cholesterol is getting to where it needs to go.
What are apoproteins?
Apoproteins are a type of protein molecule that acts as the captain of the lipoprotein vehicle. They guide the lipoprotein to where it needs to go and help regulate what it ultimately does with its cargo.
What types of apoproteins are there?
There are several types of apoproteins, each associated with different classes of lipoproteins based on size, composition, and function. The two most important ones are:
apoB, which is primarily attached to lipoproteins that are larger and have higher concentrations of cholesterol and triglycerides relative to protein.
apoA-l, which is primarily attached to lipoproteins that are smaller and have lower concentrations of cholesterol and triglycerides relative to protein.
So where do HDL and LDL come in?
Great question. HDL and LDL stand for High Density Lipoproteins and Low Density Lipoproteins, respectively.
Density is just mass divided by volume and if you remember from any introductory health class that muscle is denser than fat, that helps frame what these names mean. The higher the proportion of dense protein relative to fat (cholesterol and triglycerides), the greater the overall density. That’s true if you assume that volume is held constant or if volume goes down with increasing relative protein, which in the case of lipoproteins it does. Actually, HDL and LDL are overly simplistic descriptors, the spectrum of size and density of lipoproteins is much larger, and scientists classify them into multiple categories beyond just HDL and LDL:
Lipoproteins that carry the apoB apoprotein include:
VLDL (very low density lipoprotein) - the biggest (by volume) and lowest density (most amount of cholesterol relative to protein)
IDL (intermediate-density lipoprotein) - smaller and slightly more dense than VLDL
LDL (low density lipoprotein) smaller and denser still
Lipoproteins that carry the apoA-l apoprotein include:
HDL (high density lipoprotein) - much smaller and the least amount of cholesterol relative to protein than the rest. There’s actually a range of HDL subtypes with varying densities and functions (e.g., HDL2, HDL3), but for now, we’ll keep things simple.
At this point, I want to explain how we can keep track of the quantity of all these particles. Understanding this is critical for understanding what actually gets measured, which we will discuss later:
Cholesterol content within a lipoprotein class, denoted as “LDL-C” and “HDL-C”. This signifies the total amount of cholesterol that’s being carried by all LDL and all HDL lipoproteins, respectively, in your blood.
Lipoprotein particle count, denoted as “LDL-P” and “HDL-P”, respectively, and is just the total number of each type of lipoprotein.
Apoprotein particle count. In particular, apoB particle count, which we will talk a lot more about later.
One important realization I had at this point was:
“Wait… so HDL and LDL aren’t actually cholesterol?!”
Yup.
People—and by “people” I mean both mainstream medical professionals and everyday laypeople—often use “HDL” and “LDL” as if they’re types of cholesterol. But they’re not. HDL and LDL are entire transport vehicles, made up of fat and protein that carry cholesterol (along with triglycerides and other lipids). And the kicker? The cholesterol they carry is the exact same molecule.
So, when you hear someone say “LDL is bad cholesterol” or “HDL is good cholesterol,” just remember: that shorthand is misleading at best. Not only are HDL and LDL not cholesterol, but framing them as good or bad misses the point of how cardiovascular risk actually works.
Even if you ask an LLM questions about cholesterol, you will see the mistake of referring to HDL and LDL as cholesterol being made (I was close to rage-quitting a few times during the research process because of this). This is a sign that a large amount of our written content in newspapers and blogs online make this mistake. Typically, only scientific papers and the like are careful and accurate about differentiating between lipoproteins (the stuff that carries cholesterol) and cholesterol itself.
In the next few sections, I’ll explain why all of this matters for your health—and why the HDL/LDL distinction is woefully inadequate for assessing cardiovascular risk.
Before we move on, let me recap what we’ve discussed so far.
Cholesterol and triglycerides serve important functions in the body. They don’t mix well with water, so they are packaged together inside of lipoproteins, which can transport them through blood. Lipoproteins have apoproteins attached to them to help steer them through the blood and regulate what happens to the cholesterol and triglycerides contained within them. The two main types of apoproteins are apoB and apoA-l. They are attached to different size and density of lipoproteins, which is how we end up categorizing them. Lipoproteins with apoB are bigger and less dense and include VLDL, LDL, and IDL, and lipoproteins with apoA-l are HDLs. In terms of measurement we can think about the actual cholesterol content (in total, or within various lipoproteins) and the particle count of various lipoproteins.
Why should we care about any of this?
This is a great question - actually, it's the only important one. If I were a better writer, maybe I would have started with this question up front. But you stuck around, so let’s keep moving along.
The bottom line is this: we don’t want atherosclerosis to lead to a heart attack or stroke.
Atherosclerosis is a slow, complex process that leads to plaque buildup inside the arteries. The process begins when a lipoprotein—usually a Low-Density Lipoprotein (LDL) particle, but also other apoB-carrying lipoproteins (VLDL, IDL)—gets retained in the wall of an artery. If that particle stays there, it causes inflammation, which triggers an immune response.
When there are not a lot of LDL particles getting retained on arterial walls, the body's immune response is able to clear out the issue. But when too many LDL particles are repeatedly getting stuck in the arterial walls, the body’s immune response becomes chaotic and backfires. The immune system tries to overcorrect with a series of responses that lead to more inflammation and ultimately plaque is formed.
The lipoprotein particles that tend to do this (LDL, VLDL, IDL, and Lp(a), more on the last one later) are all considered “atherogenic”, meaning they promote the formation of atherosclerotic plaques.
But why do these particles get retained in the first place? The full picture isn’t completely understood, but the most widely accepted explanation is simple: the more atherogenic particles you have in circulation, the greater the chance one will slip through the cracks and get lodged in the arterial wall. It’s a numbers game. The endothelium (the inner lining of the artery) can usually handle a small number of these particles slipping through, but once the volume gets too high, the system becomes overwhelmed, inflammation escalates, and plaque starts to form.
And that’s why we care. If a plaque ruptures or grows large enough to significantly block blood flow, it can cause a heart attack (if it's in an artery feeding the heart) or a stroke (if it’s in an artery going to the brain).
And the key word here is “slow.” Atherosclerosis builds silently over decades. Waiting until your Medicine 2.0 doctor decides you have “early signs” of atherosclerosis in your 40s or 50s is already way too late. By the time plaque is visible on scans the process is well underway. That’s why applying a Medicine 3.0 approach—prevention through early and targeted data—is critical.
Before we move on, let’s define a few important terms that often get used interchangeably:
Atherosclerosis: The specific process of plaque buildup inside artery walls due to retained lipoproteins and inflammation. It’s the underlying cause of most cardiovascular events.
Cardiovascular Disease (CVD): A broad umbrella term that includes any disease of the heart and blood vessels. This includes atherosclerosis, heart failure, arrhythmias, and more.
Coronary Heart Disease (CHD): A subtype of CVD that specifically refers to disease of the coronary arteries—i.e., the arteries that supply blood to the heart muscle. It’s the most common type of heart disease and a major consequence of atherosclerosis.
Atherosclerotic Cardiovascular Disease (ASCVD): A clinical term that refers specifically to cardiovascular events (like heart attacks and strokes) that are caused by atherosclerosis.
Going forward, I’ll primarily use “ASCVD” when discussing how to measure or address disease risk. While many of the studies I reference report outcomes in terms of CVD or CHD, I see these as part of the same broader picture. Rather than switching terminology with every citation, I’ll stick with ASCVD throughout to keep things clear and consistent.
“Wait… so LDL is bad afterall? You tricked me!!”
No, I did not!
LDL is necessary to supply cholesterol throughout the body for the various critical functions mentioned earlier. So LDL is good. What’s bad is when too many LDL particles get retained in the walls of your arteries and trigger an inflammatory cascade.
That’s the real problem: not cholesterol in general, not even LDL cholesterol specifically—but an excessive number of LDL particles getting stuck in arterial walls. This is the root of atherosclerosis. Everything else is secondary.
So how do we prevent LDL particles from getting retained in the first place? To answer that, we need to:
Define everything we could theoretically measure in the blood,
Identify which of those measures are actually testable and meaningfully linked to ASCVD,
Understand what levels we should be aiming for, and
Know what actions to take if they’re off.
But First, a Quick tangent on Lp(a)
I know—this is a lot. But before we move on, we need to briefly talk about Lipoprotein(a), or Lp(a).
Lp(a) is essentially a special subtype of LDL. It’s just like a regular LDL particle, but with an extra attachment: a protein called apolipoprotein(a). This little add-on makes Lp(a) uniquely dangerous. It’s more likely to get stuck in arterial walls and it has pro-thrombotic properties—meaning it can promote blood clot formation.
So yeah… it’s kind of like LDL’s evil cousin.
That’s all you really need to know for now—but we’ll circle back to Lp(a) later on.
What can we measure?
Now that we understand what lipoproteins are and what they carry, let’s talk about what we can actually measure in the blood.
Lipoproteins transport cholesterol and triglycerides, and come in different forms—each with its own properties. So theoretically, there are quite a few things we could track:
Total cholesterol (TC): The total cholesterol content across all lipoproteins in the blood.
LDL-C, VLDL-C, and IDL-C: The amount of cholesterol contained specifically within each apoB-carrying lipoprotein.
HDL-C: The cholesterol content within apoA-I lipoproteins (HDLs).
LDL-P, VLDL-P, and IDL-P: The particle count of each apoB-carrying lipoprotein.
HDL-P: The particle count of HDL lipoproteins.
ApoB and ApoA-I levels: A standardized and accessible proxy for the total number of the lipoproteins they’re attached to.
Lp(a) particle count
All the same measures above for Triglycerides (where applicable)
Various ratios of any of these (LDL-C/HDL-C, TG/HDL-C, apoB/apoA-I, etc.)
Altogether, that’s over 20 individual markers, and easily hundreds of possible ratios you could analyze. Yet your standard cholesterol panel only gives you a small handful.
Am I suggesting we need to measure every single one of these? Absolutely not.
But we do need to figure out which ones actually matter—specifically, which of these markers are the most predictive of ASCVD. That’s what we’ll tackle next.
Which of the measures actually matter?
I’m going to put the measures into two tiers based on how useful they are at either predicting ASCVD or at giving useful/actionable data. For each tier, I will provide and summarize the supporting evidence for my claims.
Tier 1 - ApoB content
Mechanistically, the best understanding of the primary cause of atherosclerosis is the retention of too many apoB-containing lipoprotein particles (LDL, IDL, VLDL, and Lp(a)) in the arterial wall. The more of these particles there are in circulation, the greater the likelihood of one becoming lodged and triggering a cascade of inflammatory responses. ApoB is the structural protein on all of these atherogenic lipoproteins, and every particle has exactly one apoB molecule. This makes apoB a simple, powerful proxy for the total number of atherogenic particles.
While direct measurement of atherogenic lipoprotein particle numbers (LDL-P, IDL-P, and VLDL-P) might be ideal in theory, those tests are more expensive, less standardized, and harder to obtain. ApoB, by contrast, is widely available, inexpensive, and well-validated.
Here are my two primary reasons why apoB content is a Tier 1 ASCVD risk measure, backed up by supporting evidence:
Reason #1: ApoB shows the strongest predictive power of ASCVD out of all commonly measured lipids, including LDL-C and Total Cholesterol.
A study from 2020 by Richardson et al. attempted to figure out which lipid traits truly caused ASCVD. They did this via a multivariable Mendelian randomization analysis. In a nutshell, what that means is they took a bunch of data from previous studies (over 400,000 participants in total) that had 1) those participants’ lipid values, 2) their long-term cardiovascular outcomes, and 3) genetic data. The third thing is the key to Mendelian randomization because it creates a natural randomized trial. For example, different genes cause people to have higher/lower LDL-C, apoB, etc., so the 400,000+ participants can be grouped based on their genetic predispositions. The conclusion: apoB was the predominant lipid parameter that predicts ASCVD outcomes. In isolation, the other lipid parameters were also decent predictors, but when multivariate analysis was done on all of the parameters together, the only one that stood out was apoB, which suggests that apoB is the main causal factor and other lipid measures are useful largely because they sometimes correlate with apoB levels (Richardson et al., 2020).
To add validity to these conclusions, another research group (Marston et al.) in 2021 studied the same population data as Richardson et al. along with 40,000 more participants from another cohort, and came to similar conclusions: “Risk of myocardial infarction may best be captured by the number of apoB-containing lipoproteins, independent from lipid content (cholesterol or triglyceride) or type of lipoprotein (low-density lipoprotein or triglyceride-rich)” (Marston et al., 2021).
One super useful paper in my exploration of this topic was written in 2019. Two major European cardiology organizations (the European Society for Cardiology (ESC) and European Atherosclerosis Society (EAS)) created a task force to investigate lipid measures and cardiovascular risk in order to update European guidelines (which, by the way, are better than the American guidelines). Basically, they threw together the smartest cardiology minds to figure out what the most rigorous research to date (as of 2019) tells us, and these were the conclusions they came to (Mach et al., 2019):
They cited a 2017 study by Ference et al., which pooled data from multiple epidemiologic cohort studies, Mendelian randomization analyses, and randomized intervention trials. Across all of these methodologies, the conclusion was consistent: lipoprotein particles themselves are a causal factor in the development of atherosclerosis (Ference et al., 2017). These types of papers (meta-analysis) are arguably the best type of evidence because they don’t rely on just one data source or research team—they combine results across populations, study designs, and time periods to paint a more comprehensive picture. That said, meta-analyses aren’t perfect. The researchers still have to decide which studies to include (and exclude); which opens the door to potential bias. Ideally, peer review helps catch any cherry-picking, but it’s still something to be aware of. That’s why I made an effort to find multiple, independent meta-analyses that reached similar conclusions. The one selected by the European task force further validated the findings of the first two I mentioned.
They updated their recommendations regarding apoB. Previously (as of 2016), their recommendation was to consider apoB as an alternative, especially for people with high triglyceride content. The new recommendation suggests apoB can be used as a primary measurement. That being said, they did not make apoB the primary measurement outright, much of the guidance is still based on LDL-C despite their recognition of apoB as a more causal factor. My best guess as to why they didn’t make it the primary measure is that LDL-C is still the more widely available test, and the majority of clinical drug trials are based on LDL-C.
Reason #2: ApoB Identifies Risk When LDL-C Misses It
ApoB as a measure provides additional benefit in identifying risk over the standard LDL-C measure. This is because LDL particles have varying size and cholesterol concentrations (we talked briefly about the cholesterol transport system being complicated - suffice it to say that LDL particles are not all one and the same, they’re constantly in flux). This means that just knowing the cholesterol content of LDL (i.e., LDL-C) does not tell you how many LDL particles you have. And this is really important because many at-risk individuals can have low LDL-C, while having many smaller LDL particles, and therefore being at high risk of atherosclerosis. For these people, LDL-C is a less meaningful thing to be concerned with, and will actually lead to a false impression of low risk. To make an analogy, imagine you are hosting a party tonight at your home and are worried your driveway won’t have room for all the cars that need to be parked. You ask your assistant (you’re an executive in this analogy, stay with me here) if you’ll be at risk of not having enough parking space. Imagine he or she responds, “there are 20 people confirmed coming tonight.” without any other context. You would fire them on the spot, wouldn’t you? Knowing that there are 20 people coming doesn’t help you determine your risk of running out of parking space, since those 20 people could all be coming in 20 individual cars, or one single bus, or maybe half the people are taking Ubers, and the other half are carpooling across three cars… Hopefully, the point here is clear that knowing the number of people coming is not as useful as knowing how many vehicles there will be. The same is true for cholesterol, and its atherogenic lipoprotein vehicles.
In statistics, this phenomenon of LDL-C not always tracking with apoB is what’s known as “discordance”. In 2024 Sniderman et al. looked at ~300,000 participants and segmented apoB levels across various levels of LDL-C and concluded the following: “High variability of apoB at individual levels of LDL-C, non-HDL-C, and triglycerides coupled with meaningful differences in 10-year ASCVD rates and significant residual information contained in apoB for prediction of new-onset ASCVD events demonstrate that LDL-C, non-HDL-C, and triglycerides are not adequate proxies for apoB in clinical care.” (Sniderman et al., 2024). For most people, LDL-C and apoB levels will be correlated, but for a meaningful segment of the population, these two metrics will be discordant. In 2020, Cao et al. investigated this discordance and, while their conclusions were not strong, the data showed that 24.7% of the cohort (4,623 participants) had discordantly high apoB (meaning apoB was considered high while LDL-C was relatively low) (Cao et al., 2020).
To summarize why ApoB Belongs in Tier 1:
Mechanistically, apoB seems like a better indicator of ASCVD risk than traditional lipid markers (TC, LDL-C, HDL-C, various ratios).
Several studies confirm the mechanistic understanding and indicate apoB is a stronger predictor of ASCVD risk than traditional lipid markers.
Even if LDL-C is usually correlated with apoB, there is enough evidence showing the frequency of discordance between LDL-C and apoB suggests that it is not as reliable of an indicator.
Tier 1 - Lp(a)
Lipoprotein(a), or Lp(a), is the other parameter I would include in Tier 1. As previously described, Lp(a) is a modified form of LDL that contains an additional protein: apolipoprotein(a). This structure makes Lp(a) more prone to arterial wall retention and also promotes clot formation, making it doubly dangerous.
The Canadians taught me a lot about Lp(a). Similar to the European task force, the Canadian Cardiovascular Society published a paper in 2021 to update their guidelines (also way better than the American guidelines) based on a thorough review of the latest research (Pearson et al., 2021). Here is what I learned about lp(a) from their rigorous review of the literature:
Lp(a) is highly genetic—sex, age, and lifestyle factors don’t seem to influence Lp(a) levels much. Instead, a single gene has the biggest influence.
The paper referenced two Mendelian randomization studies that showed a strong association between Lp(a) and ASCVD risk.
There are no clear lifestyle factor changes that can reduce Lp(a), and most common lipid-lowering drugs don’t influence it either.
The ultimate recommendation is to measure this once in your life (ideally early) to help understand whether you are at higher risk. For example, if you take two people with identical lipid measures that are borderline problematic, but one person has high levels of Lp(a) and the other has low levels, the treatment plan would be totally different. The person with low levels of Lp(a) may be advised to make a number of lifestyle changes and continue to monitor things before introducing any drug treatment. Conversely, the person with high levels of Lp(a) may be put on a faster track towards considering drug treatment.
Tier 2 - well, everything else…
In my opinion, every other lipid measure can be shoved into Tier 2. That doesn’t mean these markers are useless—just that the evidence doesn’t support them being as useful or predictive as Tier 1.
Still, these markers can provide helpful context. I’ll explain what each one tells us and why it falls short compared to apoB or Lp(a).
LDL-C (cholesterol content within LDL particles)
Why is it important?
In my view, the main reason to measure LDL-C is not because it's valuable in itself, but because everyone else thinks it is. Your doctor’s playbook and many guidelines (for lifestyle and drug recommendations) are based on LDL-C.
LDL-C has been studied forever and the data undeniably shows correlation between high LDL-C and ASCVD risk. I’ve already argued why apoB does this way better, but regardless LDL-C is pretty good.
You may have the genetics that I discussed earlier that would make your LDL-C and apoB values discordant. Measuring LDL-C along with apoB is the easiest way to know that, and knowing it may influence how your doctor evaluates your lipids moving forward.
Why is it not Tier 1?
Several of the studies and cardiovascular organizations I referenced earlier have concluded that LDL-C is not as powerful as apoB.
HDL-C (cholesterol content within HDL particles)
Why is it important?
It can be used to measure your non-HDL-C levels (i.e., the cholesterol contained within all other lipoproteins that aren’t HDL, which would be more than just LDL-C as it would also include IDL and VLDL cholesterol levels). This is actually more useful than LDL-C itself, but still not as useful as apoB. As a measure itself, HDL-C is not that important, as I will argue next.
Why is it not Tier 1?
The main reason people care about HDL-C is because they think of it as the “good” cholesterol that helps in reducing your “bad” cholesterol levels. HDL is definitely involved in the overall cholesterol transport system, but raising your HDL-C levels doesn’t reliably help your ASCVD risk. In fact, big pharma has tried for the past 2 decades to develop drugs to raise HDL-C and reduce ASCVD risk. In every single case, while they were able to raise HDL-C pharmacologically, none of the trials showed a reduction in ASCVD risk, and a number of them had to be cut short as they actually increased risk. The takeaway: There’s not much we can do with HDL-C, so I don’t see much point in measuring or worrying about it.
Razavi et al. in 2023 evaluated the current literature to understand the association between HDL-C levels and ASCVD risk. They called into question the long-held belief that low HDL-C is necessarily bad, though they still acknowledge several studies that do show that association. They discuss several lifestyle factors that can increase HDL-C; in my opinion, none of them are significant enough to worry about, and in any case, most of them are the same things you would do to decrease LDL-C and apoB. They acknowledge the same thing I highlighted above regarding the failure to show a benefit from pharmacologically increasing HDL-C. Finally, they point out that at very high levels of HDL-C we begin to see increased risk of ASCVD (Razavi et al., 2023).
Examples of failed drugs:
Torcetrapic was studied in 2007 on a cohort of 15,067 patients for 12 months. It was successful in increasing HDL-C by a whopping 72.1% and reducing LDL-C by 24.9%. It also increased the risk of cardiovascular events and death compared to the control group. As a result, the study was terminated early. (Barter et al., 2007).
Another trial was attempted with Niacin in 2011. 3,414 patients were split into two groups—one group received a statin (LDL-C-lowering) treatment plus placebo, and the other received the statin and Niacin, which was supposed to increase HDL-C. After two years the Niacin group increased their HDL-C by 20%, but saw no improvement in cardiovascular outcomes. The trial was ended after three years due to lack of efficacy. (AIM-HIGH Investigators, 2011).
Roche, Eli Lilly, and Merck all attempted similar trials with their own versions of HDL-C targeting drugs, and none of them came up with anything that meaningfully reduced ASCVD risk.
Triglycerides
Why is it important?
Triglycerides have been shown to be associated with insulin resistance and more generally metabolic syndrome. Insulin resistance is basically a precursor to type 2 diabetes—it's a condition where your body doesn’t respond normally to insulin. Metabolic syndrome is a catch-all classification that refers to several physical conditions that all increase the risk of ASCVD.
This study showed correlation between triglyceride levels and several markers of Metabolic Syndrome (Tao et al., 2016).
This 2010 meta-analysis reviewed 87 studies with a total of almost 500,000 patients and found a strong association between metabolic syndrome and increased risk of ASCVD (Mottillo et al., 2010).
Why is it not Tier 1?
Similar to the rest, the overwhelming body of literature does not point to Triglycerides as being a useful measure for predicting ASCVD risk compared to apoB. To the extent that it can be useful in evaluating metabolic syndrome, it does have some value.
VLDL-C
Why is it important?
Some studies show that VLDL-C is more useful than LDL-C. But, both are still less useful than apoB (I feel like a broken record). It's an interesting additional thing to test to get an overall picture (i.e., it can explain why you might have discordance between LDL-C and apoB—if you have lots of big VLDLs, your apoB could be high despite having lower overall cholesterol).
Why is it not Tier 1?
See the last explanation, it applies here as well.
Enough Theory—Here’s How to Act on It
Okay, so now that you're basically an expert on all things cholesterol, how can you proactively take control of your health with smart lipid monitoring and management? I’m glad you asked. Here's my overview of a practical, actionable “battle plan,” which I’ll expand on in the sections that follow:
Step 1: Go to your doctor. (Seriously.)
I’m not sure if I mentioned this yet, but I am not a doctor. My recommendation now and always will be to work with your doctor and follow their guidance.
That said, the reason I wrote this article is because—after repeated attempts to find a “good” general physician—I’ve been repeatedly disappointed by the lack of proactive, preventive care. This series is my attempt to dive deep into the things I can do myself to practice a more modern, prevention-first approach to health. But even so, I always run my results and ideas by a doctor, and I continue searching for one who aligns with the Medicine 3.0 philosophy.
Step 2: Order the following blood work.
See the “How to Order Blood Work” section at the end for how and where you can order your own blood work. I'll link the ones I specifically got here.
Apolipoprotein B (ApoB)—https://www.ultalabtests.com/test/apolipoprotein-b-apob
The following five tests I got in the same bundled panel, but you could also get them individually—https://www.ultalabtests.com/test/high-risk-heart-health-lipid-and-lp-a-panel
Lipoprotein A (Lp(a))
LDL-C
HDL-C
Non-HDL Cholesterol
Triglycerides
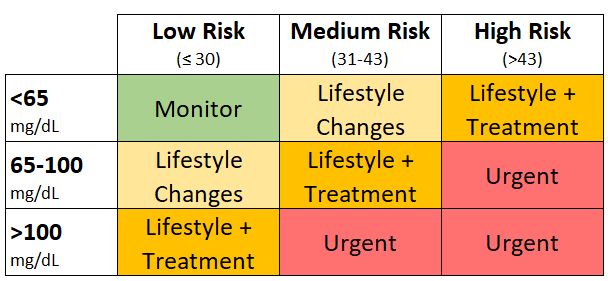
Step 3: Assess your overall risk in two dimensions.
I have developed a matrix framework based on these two dimensions that will inform Step 4.
A general ASCVD risk framework that determines your level of risk based on various factors.
The results of your blood work.
Step 4: Take action to address the results determined from step 3.
Okay, now that you’ve gone to your doctor and ordered your blood work, let’s jump right into step 3.
There are nearly a dozen formal risk calculators in circulation for assessing ASCVD or general CVD risk—tools like the American ACC/AHA Risk Estimator, the Framingham Risk Score, QRISK3 (UK), and the European SCORE2 framework. After digging through these, I found SCORE2 the most compelling—it incorporates age, sex, smoking status, systolic blood pressure, and total/non-HDL cholesterol.
The SCORE2 system requires a series of European region-specific risk charts and a mix of lifestyle and lab data. Overall, it's not very practical, especially if you’re not from Europe. I wanted a more simplified system—one where you could first determine your general risk tier (based on a simple assessment of background/lifestyle factors), and then use your blood work separately to interpret that tier more precisely. So, I built a scoring matrix. It’s not perfect, but it draws from the logic of SCORE2 and similar tools while staying more flexible and easier to apply.
Do you have a family history or genetic predisposition that would indicate heightened ASCVD risk?
Parent/sibling with a heart attack or stroke, OR your Lp(a) is > 75 nmol/L (30 mg/dL) → +28 points
Otherwise → 0 points
Are you a smoker?
Yes → +29 points
No → 0 points
Gender
Male → +17 points
Female → 0 points
Do you have high blood pressure?
Taking BP meds, OR Not medicated, but Systolic blood pressure > 140 mmHg -> +14 points
Otherwise → 0 points
Age
Over 55 → +13 points
40 - 55 → +6 points
Under 40 → 0 points
Now, add up your points:
≤30 points → Low Risk
31–43 points → Medium Risk
>43 points → High Risk
I manually tested all 48 possible combinations of these inputs against SCORE2’s risk tables and found that this system maps well to their risk groupings (being slightly more conservative for good measure).
Once you know your relative risk level, you can more accurately evaluate the one risk metric that I think matters most: apoB. I’ve based the following recommendations on the European guidelines (Mach et al., 2019) for target apoB levels in moderate, high, and very high-risk patients. In my opinion, this is the most conservative and evidence-aligned approach compared to other major guidelines.
Note: This matrix is not a clinical tool or diagnostic framework. It’s just a way to turn lab results into a conversation starter with your doctor — and to help you take the next step with clarity.
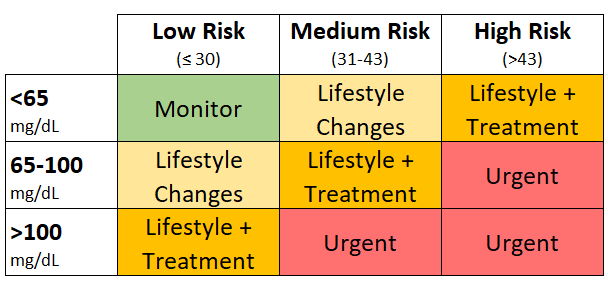
Depending on where you land in the matrix you will be one of four tracks:
Monitor: you are at low risk and have good apoB levels. There's no urgent need to change anything. Of course, following the recommended lifestyle changes and consulting with your doctor are still good ideas.
Lifestyle Changes: you are at relatively low risk and have moderate apoB levels. If your doctor is anything like mine, they will literally tell you to change nothing. I disagree; I think if you’re in this moderate range, it is appropriate to start implementing the lifestyle changes that I will describe in the next section.
Lifestyle + Treatment: Now you’re entering a zone of moderate overall risk and moderately elevated apoB. At this stage, it’s time to get serious. If your doctor isn’t taking your risk seriously, it’s worth finding one with more expertise in lipidology. At a minimum, you should be discussing lifestyle changes and increasing the frequency of blood work — but many clinicians will begin considering medications at this point. Again, if they have a “do nothing” approach, this would be a good sign to find a new doctor.
Urgent Treatment: here you are in the danger zone. You should not only be seeking out medical professionals with lipidology expertise, but you should basically not accept anyone who isn’t putting you on a drug treatment plan. I would recommend reading Section 8 of the European Guidelines report (Mach et al., 2019) several times—it covers the most up-to-date (as of 2019 at least) pharmacological treatments available. Obviously, your doctor should be the one determining the best drug treatment plan for you, but the more knowledgeable you are, the better you can determine if your doctor is well-informed. For example, if I were in this category and my doctor wasn’t aware of PCSK9 inhibitors and only knew about statins, then I would find a new doctor. To be clear, I don’t think everyone in this category necessarily needs to be on PCSK9 inhibitors, but if your doctor doesn’t even know about them, it is a clear sign they are not caught up with the latest drug research, and I would want to find a doctor who is.
Lifestyle Changes to Lower ASCVD Risk
Okay, so if you fall into any of the categories that suggest making lifestyle changes, here is what you can do (hint: every category technically could benefit from these).
Smoking
Smoking significantly increases cardiovascular risk. This paper covers the topic quite well; I’ll go over the main points here (Gallucci et al., 2020):
There are numerous studies that show an association between smoking and a negative impact on lipid markers (higher LDL-C, higher TC, higher Triglycerides, and lower HDL-C).
There are numerous studies showing smoking increases the rate of heart attacks and ASCVD-associated deaths.
While we don’t know the precise mechanism that links smoking to these things, the basic theory makes a lot of intuitive sense. Smoking, through a number of pathways, severely damages the health of your endothelium—i.e., the lining of arterial walls. And if you remember, atherosclerosis starts with lipoprotein particles (mainly LDL) embedding themselves in that lining and eventually triggering a cascade of events that lead to plaque formation. The hypothesis here is that the damage that smoking causes just magnifies the atherosclerotic process.
Smoking is a personal choice—but if lowering your ASCVD risk is a priority, quitting is one of the most powerful things you can do.
Nutrition
Dietary Cholesterol
First, I want to talk about dietary cholesterol, since that may seem like an obvious place to start. Ironically, reducing dietary cholesterol is not very important. The vast majority of the cholesterol in our body is synthesized by our cells (Corliss, 2019). So, practically speaking, reducing your dietary cholesterol intake is not going to do much. Since that’s a very bold and controversial claim that a lot of people may doubt, let me back it up with evidence and you can decide for yourself if you agree:
A meta-analysis from 2015 took a comprehensive look at the relationship between dietary cholesterol and ASCVD (Berger et al., 2015). The analysis surveyed 40 studies with a total of 360,000 participants that had been analyzed from 1979 to 2013. Each study that was analyzed in this meta-analysis had data on dietary cholesterol intake (with at least a low and high group) and studied both ASCVD outcomes and lipid measures. Before I continue, I want to acknowledge that this meta-analysis was in part sponsored by the American Egg Board. Some people might scream that that makes the study invalid. To those people, I would suggest two things: 1) every single study ever done is sponsored by someone, so unless you want to throw out all of scientific literature as invalid and biased, you’re going to need to get over this view; and 2) there’s nothing stopping you from reading every single study that was included (and excluded) from this meta-analysis to see if you would come to a different conclusion (I read many of them to stress-test my conclusions). Here are the main takeaways:
First, the paper looked for any associations between dietary cholesterol intake and any type of ASCVD risk/event, including fatal and nonfatal Coronary Artery Disease, and different types of strokes. In total, it looked at 34 studies and found 23 that found no association at all, and 11 that had some statistically significant association between dietary cholesterol and ASCVD risk/events.
Next, the paper looked for any association between dietary cholesterol and changes in serum lipid levels. The results require some nuance to fully understand. When looking at 18 studies individually, they found an average statistical increase in total cholesterol of about 0.008 mg/dl increase in serum cholesterol for every 1 mg increase in dietary cholesterol. To put that in context, one egg has roughly 190 mg of cholesterol, which would come out to a total cholesterol increase of 1.6 mg/dl (with about half of that being LDL cholesterol). However, very importantly, this relationship went away when dietary interventions exceeded 900 mg of daily cholesterol intake. Which means that for the first five eggs you eat in a day, you may see a total increase of 8 mg/dL in your total cholesterol (roughly 4 mg/dL increase in LDL-C), and then beyond that, no noticeable change. Keep in mind that eggs are just one source of dietary cholesterol; there are similar levels in butter, meat, and seafood. Furthermore, when the researchers did a meta-regression analysis across all the studies together, they found no linear relationship between dietary cholesterol and serum lipid levels.
My sense is the following: the data on dietary cholesterol association with ASCVD and serum lipid levels is murky. Not only are there dozens of studies with disparate findings, but the quality of studies is questionable (it is extremely hard to accurately control and measure dietary cholesterol levels, and the vast majority of these studies are based on subjects answering questionnaires about their diet—which is obviously unreliable). Given that the totality of evidence doesn’t show a strong linear relationship and that individual studies that do show an association show a relatively small increase in serum lipids with a pretty low level where the association plateaus, I do not personally believe dietary cholesterol is the right area to focus on, especially since we have other dietary factors where the relationship is much clearer.
Saturated Fat
On the other hand, saturated fat is a nutritional vector that makes sense to target.
In 2023, the World Health Organization (WHO) did a meta-analysis including data from studies up to 2020 on the effects of saturated and trans fats on cardiovascular health (Reynolds et al., 2022). They did this to help inform the WHO dietary guidelines for reducing cardiovascular disease risk. They looked at a variety of data points, including the type and source of fat, as well as the effect of replacing the fat with different macronutrients. Overall, the meta-analyses contained over one hundred studies with millions of total participants. This was the highest quality and most recent meta-analysis I could find on this topic. Here are the notable conclusions:
Replacing 5% of your daily total caloric energy (TE) worth of Saturated Fatty Acids (SFA) with an equivalent amount of Polyunsaturated Fatty Acids (PUFA), Monounsaturated Fatty Acids (MUFA), or carbs reduced overall risk of death by 15%, 16%, and 8%, respectively. While replacing 2% TE of SFA with trans fat (TF) resulted in a 9% increase in overall risk of death.
Replacing 5% TE of SFA with PUFA, plant-based MUFA, or plant-based protein reduced risk of ASCVD outcomes by 11%, 17%, and 17%, respectively. Interestingly, when they compared slow-digesting carbs to fast-digesting carbs, they saw a change in risk of -6% (risk reduction) and +8% (risk increase)—meaning that if you replace SFAs with slow-digesting carbs, you can reduce your risk, but if you replace them with fast-digesting carbs (i.e., most processed carb foods), you will increase your risk.
Conclusion: both SFA and TF are associated with death and ASCVD. Shifting energy away from SFA and TF and replacing it with either PUFAs, plant-based MUFAs, or slow-digesting carbs seems to have a significant impact on reducing risk.
Another meta-analysis that I found noteworthy was completed in 2003 by Mensick et al. There are two things I really liked about this paper. First, it only included studies that kept cholesterol intake constant, which I think is really important since a lot of foods high in SFAs are also high in cholesterol. By keeping cholesterol intake constant between high and low SFA groups, the results can more reliably conclude that any observed impact is from SFA and not cholesterol consumption. The second thing I really liked about this study is that they looked at apoB levels! Specifically, the study looked at what happens when you replace 1% of total caloric energy from carbs in your diet with either PUFA or SFA. The results showed that for both apoB and LDL-C, you can reduce your levels by shifting calories from carbohydrates to PUFAs, and conversely, you will increase your levels if you replace those carbs with SFA. Roughly speaking, if you replace 75g of carbs with 33g of PUFA (calorically these are equivalent), you can decrease both your LDL-C and apoB by about 10 mg/dL. If you instead replace those 75g of carbs with 33g SFA, you will increase your LDL-C by about 18 mg/dL and your apoB by about 3.9 mg/dL. (Mensink et al., 2003).
As far as hard recommendations, the WHO ultimately recommends consuming less than 10% of TE from SFA and less than 1% from TF. Now, this is based on the WHO’s review of many meta-analyses that compared higher and lower SFA and TF consumption groups. A lot of their analysis was based on groups that were above and below 10%, but there were some studies that showed additional benefit going even further (down to 8%). I think 10% is a fine target, but going lower will be better. For context, 10% of a 2,000-calorie diet equates to about 22g of SFA (World Health Organization, 2023).
So, to conclude, we have various meta-analyses that have looked at hundreds of individual studies over the last 50+ years and have found that moving calories away from SFAs and TF and into PUFAs can reduce both the risk of ASCVD events and improve your LDL-C and apoB markers significantly.
Fiber, Fruits, and Vegetables
There are not many foods that will really improve lipid markers, but there are a few.
Soluble fiber in general. In a 2022 paper, Fu et al. analyzed 52 different meta-analyses that all looked at dozens of studies on soluble fiber (Fu et al., 2022). All the results in that paper are in relevant terms, but my ballpark math concludes that 10g of additional soluble fiber (about three servings of oatmeal) can reduce LDL-C by about 10 mg/dL.
As far as hard recommendations, most countries' health agencies recommend somewhere between 25-40g of daily soluble fiber (Miller, 2020). I’d say, shoot for the upper end of that range. For context, the average American diet has 16.5 g of fiber. So, going from the average of 16.5g up to 40g could potentially lower LDL-C by more than 20 mg/dL (obviously that’s not guaranteed, but the data suggests that it's possible).
Fruits and vegetables… This should be pretty obvious, but fruits and veggies are good for you. Maybe that’s not obvious to the carnivore crowd. I will admit it’s very hard to piece out what’s actually making the difference—is it the vitamins and minerals from the fruits and veggies? Is it the fiber? Is it just the displacement of calories from SFA/TF and refined carbs and into fruits/veggies? Who knows. One meta-analysis at least showed a small but significant reduction in heart disease, cancer, and all-cause mortality risk from eating up to 800g of fruits and veggies per day (Aune et al., 2017).
Supplements
The two supplements that are often discussed for lipid management are fish oil and berberine.
The European review paper I previously cited discusses both quite well (Mach et al., 2019). The TLDR on fish oil is that most of the studies show a trivial impact on lipids and overall disease risk (though they do significantly lower triglycerides somehow).
Berberine is lacking a lot of robust studies. One 2015 meta-analysis shows some promising results, but it only included a total population of 2,569 participants across 27 studies (Lan et al., 2015).
I personally take a fish oil supplement because it has other health benefits and seemingly no major risks, but I’m not expecting it to have any major impact on my lipid markers. I would consider taking berberine if, after deploying all lifestyle changes, I still have room for improvement in my lipids, but not quite at the level of needing pharmacology. For everyone else, based on the evidence, you can skip the supplements, do the lifestyle stuff, and jump straight to pharmacology as soon as you need it (i.e., as soon as your doctor says so).
Exercise
I won’t spend much time on exercise—it should be obvious that it's beneficial for heart health. That said, I couldn’t find much robust evidence suggesting that it significantly improves LDL-C or apoB. One study by Holme et al. reported about a 10 mg/dL reduction in apoB after one year of exercise (Holme et al., 2007). That’s promising, but it was a single study with just 219 participants. Compare that to the hundreds of thousands of participants analyzed across dozens of nutritional meta-analyses, and it’s clear the evidence base isn’t nearly as strong.
Still, the broader health benefits of exercise are undeniable. For this discussion, its biggest impact is likely on metabolic health—particularly insulin sensitivity and triglyceride levels—which indirectly lowers ASCVD risk.
Bottom line: exercise as much as possible.
To summarize the lifestyle things we can do:
Quit smoking entirely if you can.
Reduce SFA and TF intake
<10% SFA (<8% is better)
<1% TF (0% is better)
Replace SFA and TFs with PUFAs and plant-based MUFAs and to a lesser extent complex slow-digesting carbs.
Increase soluble fiber in general, and fruits and vegetables, specifically.
Fiber: 25-40g (shoot for 40g!)
Fruits/Veggies: 400-800g
Consider Supplements:
Fish oil, though it likely won’t do much.
Berberine - definitely run it by your doctor, but it could be beneficial.
Exercise!
Let’s take a look at a relatively standard American diet (this is probably considerably healthier than the actual average American diet) with a total daily calories of 2,500 (which would be roughly around maintenance calories for an active young male—you’ll need to adjust this up/down based on your activity, gender, age, weight/height, etc.).
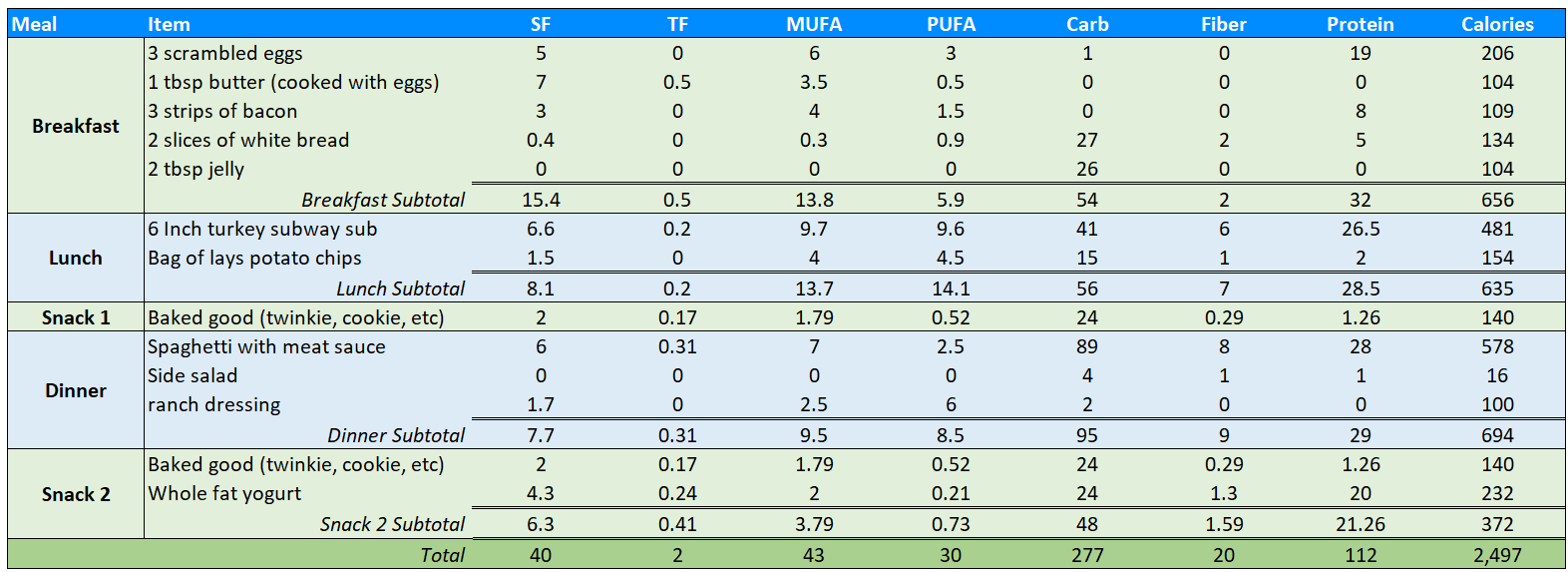
Let’s compare that to our optimal targets:
The 40g of saturated fat comes out to around 14% of total calories, well above our 10% target.
The 2g of trans fat is just under the 1% target, so that’s good. Turns out it's quite hard to eat lots of trans fat if you put in at least some effort to eat “healthy”.
20g of fiber is well below the ideal.
The only fruits and veggies come from whatever is on the sub (lettuce, peppers, onions, etc.) and the side salad—well below the 400g minimum.
Here are some suggestions that make this diet more optimal for ASCVD risk management:
Cut out the high-saturated-fat animal foods like butter, bacon, red meat entirely, and replace them with healthier options.
Instead of butter, use avocado or extra virgin olive oil.
Instead of bacon for breakfast, you can get more protein from a nonfat Greek yogurt bowl.
Instead of red meat, try fish or plant-based proteins like lentils, beans, or quinoa.
Replace the processed carbs with fruits and veggies.
Instead of toast with jelly, have a bowl of fruit with yogurt.
Instead of chips and baked goods as snacks, have snackable fruits and veggies, like carrot sticks, peaches, apples, etc.
Instead of a side salad with ranch, make a real salad with lots of greens and a homemade dressing from olive oil and vinegar, or eat a large serving of cruciferous vegetables (like broccoli, asparagus, Brussels sprouts, cauliflower, etc.)
Implementing each of these changes could look like this:
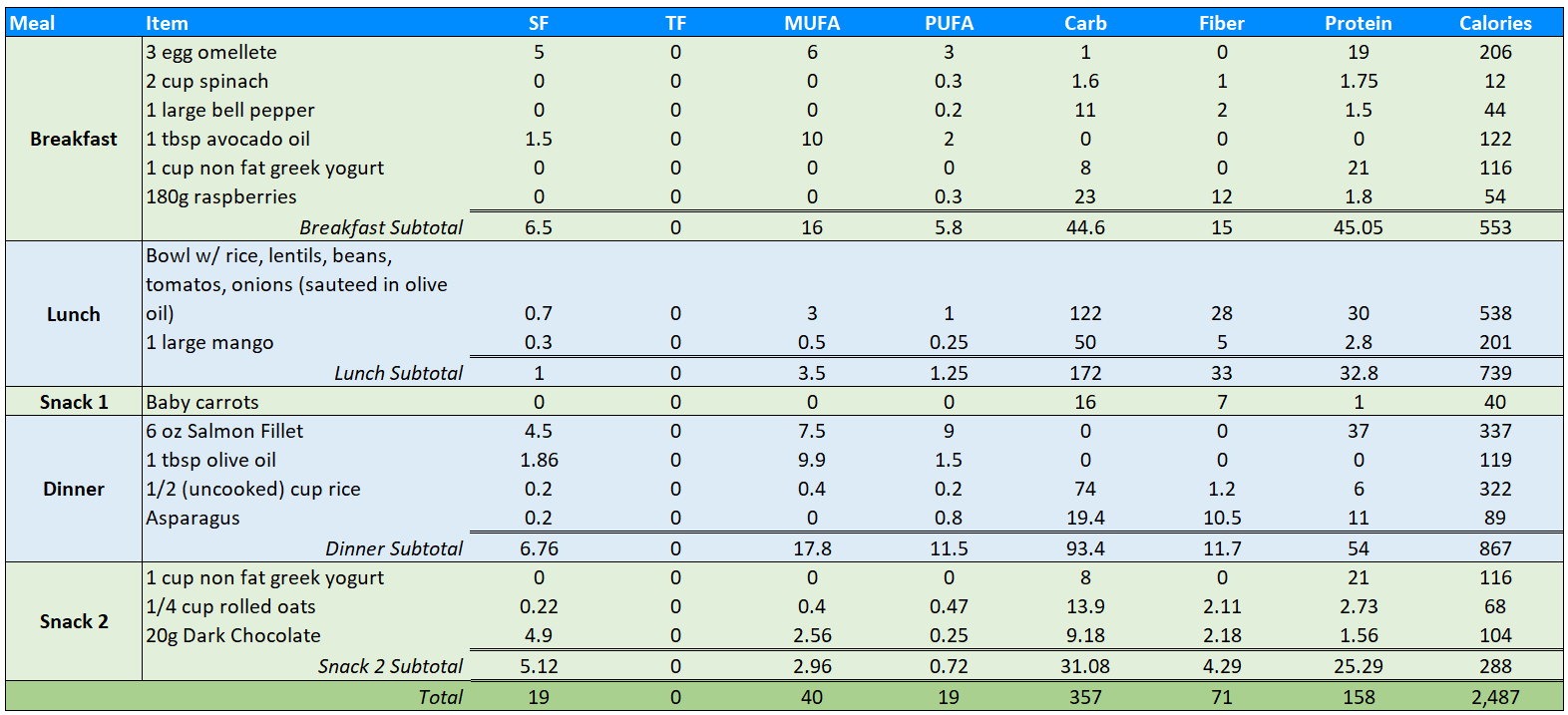
Notice that with only a few changes we’ve made massive improvement on our nutritional targets:
Saturated fat down to 19g comes out to 7% of total energy, below our 10% target.
0g of trans fat now is excellent.
Fiber is at 71g! Well above our target range of 25-40g, which is great!
Our total fruit and veggie consumption is now over 800g!
Additionally, for the same amount of calories, we’re getting 46g more of protein for a total of 158g—which is great for an athletic young adult (ideal protein targets should be discussed with a physician as certain conditions may warrant eating less protein).
Note: None of this should be taken as literal dietary advice, as diets are extremely individual and need to be discussed with a healthcare professional. The above examples are merely to demonstrate how the conclusions from the data can be implemented in a hypothetical diet.
Pharmacology and Finding a Good Doctor
I don’t know if I’ve mentioned this, but I am not a doctor.
While I believe many general physicians in the U.S.—at least the three I’ve personally evaluated—are not up-to-date on the latest lipidology research or preventive care guidelines, I still think it’s incredibly important to find a good doctor you can trust to help you navigate cardiovascular risk.
If you’re in the Medium or High risk bucket according to my framework and you find yourself in either the “Lifestyle + Treatment” or “Urgent Treatment” categories, then you might be wondering how to actually find a doctor who’s competent in this area. A few tips:
First, finish this article. You’re already well on your way to having a solid understanding of lipidology, which will help you evaluate whether a doctor truly knows what they’re talking about.
Second, ask your doctor to test for apoB and Lp(a) along with the standard lipid panel. If they refuse—or brush you off with comments like “those tests aren’t necessary” or “that’s overkill”—I’d personally consider finding a new doctor. There are enough global guidelines and expert consensus documents from top cardiology organizations stating clearly that these are more informative markers than what’s on a standard panel. If your doctor doesn’t know that, they probably haven’t read much lipidology literature lately. That’s not meant to be a dig—general physicians are busy and can’t be experts in everything—but this is your life, and you don’t need to rely on someone who’s behind on the science.
Third, learn the basics of the pharmacological options. You don’t need to design your own drug treatment plan—I certainly wouldn’t—but you should know enough to gauge whether your doctor is well-informed. For example, if a doctor is only familiar with statins and has no idea what PCSK9 inhibitors or ezetimibe are, that would be a red flag for me. Statins are excellent, and probably the foundation of most lipid-lowering regimens. But some of the most promising results in recent years have come from combination therapies. I’d want a doctor who knows that.
I highly recommend reading Section 8 of the European Guidelines on Cardiovascular Disease Prevention (Mach et al., 2019)—it’s an excellent overview of the evidence on lipid-lowering pharmacology. But if you’re short on time, here’s the bare minimum you should know:
Statins
Statins are the most common drug to treat dyslipidemia. They work by inhibiting an enzyme involved in cholesterol production in the liver.
Statins work very well. A normal dose can reduce LDL-C by 30–50%. More importantly, that reduction translates to a real reduction in ASCVD events—unlike HDL-C-raising drugs, which improve blood work but don’t improve outcomes.
For the most part, statins are very well tolerated with minimal side effects.
Ezetimibe
Ezetimibe works very differently than statins—it lowers the absorption of cholesterol in the small intestine (the cholesterol from your food and from bile, which is your own recycled cholesterol). This reduction in absorbed cholesterol is noticed by the liver, which causes it to pull more LDL particles out of the blood to compensate, which overall reduces the blood LDL-C (and likely overall apoB count) in the blood.
Ezetimibe on its own can reduce LDL-C by about 15–20%, and when it is paired with statins, it can reduce LDL-C by an additional 20–27%. So, a total of 50–75% when both drugs are taken together. Some studies have shown that the additional decrease in LDL-C in the combined therapy has led to a reduction in ASCVD risk when compared to statins alone.
No major side effects.
PCSK9 Inhibitors
The liver has LDL receptors that remove LDL particles from the blood and break down their cholesterol content. PCSK9 is a protein that marks these receptors for destruction. PCSK9 inhibitor drugs are a type of monoclonal antibody that bind to the PCSK9 protein and prevent it from marking the LDL receptors, which in turn causes more LDL particles to be cleared from the blood by the liver.
When PCSK9 inhibitors are taken with statins, they can decrease LDL-C by 46–73%.
PCSK9 inhibitors are the newest drug treatment option compared to the other two. The trials that have recently finished have shown that it can reduce ASCVD outcomes by 15–20% compared to just statins alone. Given the cost of PCSK9 inhibitors and the limited long-term data, they are typically only used in ultra-high-risk patients.
I’m still looking for a doctor I trust. I’ve already been through three GPs in the last two years, and I’m taking a break until next year. Also, I’m in the low-risk group, so there’s less urgency for me.
When I do start again, I’ll be searching for general physicians within 50 miles who have some background in lipidology or cardiovascular care—via residencies, academic work, or patient reviews. I’ll keep going until I find one who doesn’t look at me sideways when I ask for an apoB test, or tell me I don’t need to test Lp(a) (which, again, is a once-in-a-lifetime test for most people).
If you’re in a higher risk category, this search is even more important. Asking your doctor about the testing and drug options is a great way to see how much they really know.
I hope none of this comes off as arrogant. Doctors are incredibly smart, and just because I’ve written this article doesn’t mean I know more than they do. But general physicians, by definition, aren’t specialists in every area. Cardiovascular risk is too important to be managed by someone who’s only read the basics.
I want a doctor who’s kept up with the latest research on testing, prevention, lifestyle, and pharmacology—because that’s the kind of person I trust with my life. ASCVD develops slowly over decades. Being told “you’re young and healthy, don’t worry about it yet” is a comforting sentiment—but it’s also how people end up with massive plaque buildup in their 40s and 50s without warning.
This is too important to leave to chance.
Conclusion: Example of How to Use this Information
I’m going to conclude by running through the steps I took after acquiring all the knowledge I have shared in this article.
Step 1: I went to my doctor. Actually, I went to three doctors. None of them wanted to get the additional lipid testing I wanted, so I ordered it myself.
Next, I did a bunch of research to write this article. Using my framework, I assessed my risk:
I don’t have a family history of heightened ASCVD risk, nor do I have an Lp(a) greater than 30 mg/dL. So, 0 points there.
I am not a smoker. 0 points.
I am male. 17 points.
I do not have high blood pressure and am not taking blood pressure medication. 0 points.
I am in my early 30s, so 0 points.
With a total of 17 points, I am in the Low risk category.
Next, I evaluated my lipids.
apoB = 100 mg/dL
Lp(a) = <10 nmol/L
Total cholesterol = 180 mg/dL
LDL-C = 122 mg/dL
VLDL-C = 10 mg/dL
HDL-C = 53 mg/dL
Triglycerides = 50 mg/dL
I included everything, but as you know, I really only care about apoB (and Lp(a), which influenced the risk framework).
With an apoB of 100 mg/dL in the low-risk category, that puts me right on the border of Monitor and Lifestyle Changes:
I did take my lipid levels to the third doctor I saw. He looked at them for five seconds and said, “Everything is fine”. When I pushed him on apoB, he argued that it wasn’t a measure that makes sense to look at until I’m older. Needless to say, I no longer go to that doctor for anything lipid-related.
In my situation, I’m going to deploy lifestyle changes for the next few months and retest my apoB to see if I can get it below 80, which I think is probably the most I can do with just diet. I’m going to shoot for the targets around SFA, TF, fiber and fruits and veggies—actually, the sample diet I laid out above is pretty close to how I eat now. If diet alone can’t get me below 80, I will look into berberine as an option for two months and see if it makes any impact.
I am going to continue to monitor all these things on a yearly basis. For my annual physical next year, I am on a mission to find a doctor who cares about preventive medicine. Wish me luck!
How to Order Blood Work
If you’re interested in taking control of your health with DIY blood testing, here’s exactly how to do it:
1. Decide What You Want to Test
Before you even look at lab test websites, figure out exactly what markers you want to check. Otherwise, you’ll quickly get overwhelmed by the endless options—and probably end up wasting money on unnecessary tests.
2. Compare Prices Across Online Lab Providers
Not all lab testing services are priced the same. After researching, I found these three companies to be the best options:
✅ Marek Health → marekdiagnostics.com
✅ Ulta Lab Tests → ultalabtests.com
✅ Own Your Labs → ownyourlabs.com
💰 Discount Tip:
Marek Health has multiple 10% off codes floating around (I used “MPMD”, but you can find others if that one expires).
Ulta Lab Tests offers a 20% first-time discount when you sign up.
I personally ordered ~70% of my tests from Ulta (because the 20% discount made it the cheapest option for most things), and the rest from Marek. Own Your Labs had one test that was slightly cheaper, but the savings were under $10, so I didn’t bother placing a third separate order. The lipid-related tests that I got cost $80 in total after all discounts.
3. Ordering & Payment (Insurance, HSA, etc.)
One downside: you can’t use insurance for these tests. If anyone knows a workaround, please share! I couldn’t find one.
However, HSA funds are allowed—so if you have an HSA, use it! That’s what I did.
4. Getting Your Blood Drawn
Once you order, the tests are processed by major lab chains:
Ulta Lab Tests → Quest Diagnostics
Marek Health → LabCorp
I scheduled both my Quest and LabCorp appointments on the same day, one hour apart. Pro tip: Wear a long-sleeve shirt and switch arms for the second draw—just in case the techs get weird about drawing blood twice in one day.
In total, I had 11 vials drawn, which might sound like a lot, but it’s really not. For reference, a standard blood donation is over 15 vials worth of blood. So, unless you're really squeamish, you'll be fine. Note: the 11 vials were for more than just lipids. If you’re only ordering lipid tests it will be about one to three vials.
References
Andrew N REYNOLDS, Leanne HODSON, Russell DE SOUZA, Huyen TRAN DIEP PHAM, Lara VLIETSTRA, Jim MANN Saturated fat and trans-fat intakes and their replacement with other macronutrients - a systematic review and meta-analysis of prospective observational studies. World Health Organization Nutrition and Food Safety https://books.google.com/books?hl=en&lr=&id=tnwOEQAAQBAJ&oi=fnd&pg=PR2&dq=trans+fat+cardiovascular+disease+meta+analysis&ots=HF7l1ebr5Y&sig=1_r3ToTJMHe1lY0UxoifSSpPiSs#v=onepage&q&f=false
Alexander C Razavi, Vardhmaan Jain, Gowtham R Grandhi, Parth Patel, Angelos Karagiannis, Nidhi Patel, Devinder S Dhindsa, Chang Liu, Shivang R Desai, Zakaria Almuwaqqat, Yan V Sun, Viola Vaccarino, Arshed A Quyyumi, Laurence S Sperling, Anurag Mehta, Does Elevated High-Density Lipoprotein Cholesterol Protect Against Cardiovascular Disease?, The Journal of Clinical Endocrinology & Metabolism, Volume 109, Issue 2, February 2024, Pages 321–332, https://doi.org/10.1210/clinem/dgad406
Allan D Sniderman, Line Dufresne, Karol M Pencina, Selin Bilgic, George Thanassoulis, Michael J Pencina, Discordance among apoB, non–high-density lipoprotein cholesterol, and triglycerides: implications for cardiovascular prevention, European Heart Journal, Volume 45, Issue 27, 14 July 2024, Pages 2410–2418, https://doi.org/10.1093/eurheartj/ehae258
Attia, P., & Gifford, B. (2023). Outlive: The science and art of longevity. Harmony.
Aune, D., Giovannucci, E., Boffetta, P., Fadnes, L. T., Keum, N., Norat, T., Greenwood, D. C., Riboli, E., Vatten, L. J., & Tonstad, S. (2017). Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. International journal of epidemiology, 46(3), 1029–1056. https://doi.org/10.1093/ije/dyw319
Berger Samantha, Raman Gowri, Vishwanathan Rohini, Jacques Paul F, Johnson Elizabeth J. Dietary cholesterol and cardiovascular disease: a systematic review and meta-analysis The American Journal of Clinical Nutrition Volume 102, Issue 2, August 2015, Pages 276-294 https://doi.org/10.3945/ajcn.114.100305
Brian A. Ference, Henry N. Ginsberg, Ian Graham, Kausik K. Ray, Chris J. Packard, Eric Bruckert, Robert A. Hegele, Ronald M. Krauss, Frederick J. Raal, Heribert Schunkert, Gerald F. Watts, Jan Borén, Sergio Fazio, Jay D. Horton, Luis Masana, Stephen J. Nicholls, Børge G. Nordestgaard, Bart van de Sluis, Marja-Riitta Taskinen, Lale Tokgözoğlu, Ulf Landmesser, Ulrich Laufs, Olov Wiklund, Jane K. Stock, M. John Chapman, Alberico L. Catapano, Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel, European Heart Journal, Volume 38, Issue 32, 21 August 2017, Pages 2459–2472, https://doi.org/10.1093/eurheartj/ehx144
Cao, J., Nomura, S. O., Steffen, B. T., Guan, W., Remaley, A. T., Karger, A. B., Ouyang, P., Michos, E. D., & Tsai, M. Y. (2020). Apolipoprotein B discordance with low-density lipoprotein cholesterol and non-high-density lipoprotein cholesterol in relation to coronary artery calcification in the Multi-Ethnic Study of Atherosclerosis (MESA). Journal of clinical lipidology, 14(1), 109–121.e5. https://doi.org/10.1016/j.jacl.2019.11.005
Corliss J. How it’s made: Cholesterol production in your body Harvard Health Publishing https://www.health.harvard.edu/heart-health/how-its-made-cholesterol-production-in-your-body
François Mach, Colin Baigent, Alberico L Catapano, Konstantinos C Koskinas, Manuela Casula, Lina Badimon, M John Chapman, Guy G De Backer, Victoria Delgado, Brian A Ference, Ian M Graham, Alison Halliday, Ulf Landmesser, Borislava Mihaylova, Terje R Pedersen, Gabriele Riccardi, Dimitrios J Richter, Marc S Sabatine, Marja-Riitta Taskinen, Lale Tokgozoglu, Olov Wiklund, ESC Scientific Document Group , 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS), European Heart Journal, Volume 41, Issue 1, 1 January 2020, Pages 111–188, https://doi.org/10.1093/eurheartj/ehz455
Fu, L., Zhang, G., Qian, S., Zhang, Q., & Tan, M. (2022). Associations between dietary fiber intake and cardiovascular risk factors: An umbrella review of meta-analyses of randomized controlled trials. Frontiers in nutrition, 9, 972399. https://doi.org/10.3389/fnut.2022.972399
Gallucci, G., Tartarone, A., Lerose, R., Lalinga, A. V., & Capobianco, A. M. (2020). Cardiovascular risk of smoking and benefits of smoking cessation. Journal of thoracic disease, 12(7), 3866–3876. https://doi.org/10.21037/jtd.2020.02.47
I. Holme, A. T. Høstmark, S. A. Anderssen. ApoB but not LDL-cholesterol is reduced by exercise training in overweight healthy men. Results from the 1-year randomized Oslo Diet and Exercise Study Journal of Internal Medicine https://doi.org/10.1111/j.1365-2796.2007.01806.x
Jiarong Lan , Yanyun Zhao, Feixia Dong, Ziyou Yan, Wenjie Zheng, Jinping Fan, Guoli Sun. Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipemia and hypertension Journal of Ethnopharmacology
Volume 161, 23 February 2015, Pages 69-81 https://doi.org/10.1016/j.jep.2014.09.049
Kevin Burke Miller, Review of whole grain and dietary fiber recommendations and intake levels in different countries, Nutrition Reviews, Volume 78, Issue Supplement_1, August 2020, Pages 29–36, https://doi.org/10.1093/nutrit/nuz052
Marston NA, Giugliano RP, Melloni GEM, et al. Association of Apolipoprotein B–Containing Lipoproteins and Risk of Myocardial Infarction in Individuals With and Without Atherosclerosis: Distinguishing Between Particle Concentration, Type, and Content. JAMA Cardiol. 2022;7(3):250–256. doi:10.1001/jamacardio.2021.5083 https://jamanetwork.com/journals/jamacardiology/fullarticle/2786333
Philip J. Barter, M.D., Ph.D., Mark Caulfield, M.D., M.B., B.S., Mats Eriksson, M.D., Ph.D., Scott M. Grundy, M.D., Ph.D., John J.P. Kastelein, M.D., Ph.D. Effects of Torcetrapib in Patients at High Risk for Coronary Events N Engl J Med 2007;357:2109-2122 DOI: 10.1056/NEJMoa0706628 https://www.nejm.org/doi/full/10.1056/NEJMoa0706628
Pearson, Glen J. et al. 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in Adults Canadian Journal of Cardiology, Volume 37, Issue 8, 1129 - 1150 https://onlinecjc.ca/article/S0828-282X(21)00165-3/fulltext
Richardson, T. G., Sanderson, E., Palmer, T. M., Ala-Korpela, M., Ference, B. A., Davey Smith, G., & Holmes, M. V. (2020). Evaluating the relationship between circulating lipoprotein lipids and apolipoproteins with risk of coronary heart disease: A multivariable Mendelian randomisation analysis. PLoS medicine, 17(3), e1003062. https://doi.org/10.1371/journal.pmed.1003062
Ronald P Mensink, Peter L Zock, Arnold DM Kester, Martijn B Katan. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: a meta-analysis of 60 controlled trials The American Journal of Clinical Nutrition
Volume 77, Issue 5, May 2003, Pages 1146-1155 https://doi.org/10.1093/ajcn/77.5.1146
Salvatore Mottillo,Kristian B. Filion,Jacques Genest, Lawrence Joseph, Louise Pilote, Paul Poirier, Stéphane Rinfret, Ernesto L. Schiffrin, and Mark J. Eisenberg The Metabolic Syndrome and Cardiovascular Risk: A Systematic Review and Meta-Analysis JACC. 2010 Sep, 56 (14) 1113–1132 https://www.jacc.org/doi/full/10.1016/j.jacc.2010.05.034
Saturated Fatty Acid and Trans-Fatty Acid Intake for Adults and Children: WHO Guideline [Internet]. Geneva: World Health Organization; 2023. Summary of evidence. Available from: https://www.ncbi.nlm.nih.gov/books/NBK594778/
Tao, L. X., Yang, K., Liu, X. T., Cao, K., Zhu, H. P., Luo, Y. X., Guo, J., Wu, L. J., Li, X., & Guo, X. H. (2016). Longitudinal Associations between Triglycerides and Metabolic Syndrome Components in a Beijing Adult Population, 2007-2012. International journal of medical sciences, 13(6), 445–450. https://doi.org/10.7150/ijms.14256
The AIM-HIGH Investigators. Niacin in Patients with Low HDL Cholesterol Levels Receiving Intensive Statin Therapy N Engl J Med 2011;365:2255-2267 DOI: 10.1056/NEJMoa1107579 https://www.nejm.org/doi/full/10.1056/NEJMoa1107579#APPNEJMoa1107579SUP